Head Injury
1. a) Define Head Injury
b) State the types and causes of Head Injury
c.) Explain the signs and symptoms of Base of skull injury
d) Discuss the management of Head Injury
Definition
Any injury resulting in trauma to the skull or brain
Causing : fractures, haemorrhages inside the skull, haematomas inside the brain or between its coverings, neuronal injuries,
Etiology (Causes)
Accidents
Assaults
falls
Many of them are minor
Clinical Features
Conspicuous or inconspicuous
Sleepiness
Abnormal behavious
Loss of consciousness
Vomiting - projectile or non projectile
Severe head ache
Altered pupil size
Reduced or absent limb movements
Classification (Types)
Injury to superficial structures like scalp, skull : closed or open
Concussion
Contusion
Intracranial hemorrhage : hematomas : subdural, subarachnoid, extradural, intraparenchymal
Contrecoup injuries - injury to the brain diametrically opposite to the site of impact
Specific Problems
Skull fracture
Lacerations to the scalp : hge
Subdural haematoma
Extradural haematoma
Subarachnoid hge
Concussion - a temporary loss of function
Cerebral contusion
Dementia pugillistica : "punch-drunk syndrome" caused by repetitive head injuries (e.g. Boxing)
Coma
Death
Shaken baby syndrome - a form of child abuse
Pathophysiology
Brain damage at the time of injury - contusion, lacerations and torn blood vessels, acceleration/deceleration
Brain damage that occurs after the injury - swelling, ongoing bleeding, build-up of pressure inside the skull - fixed space which does not expand to allow swelling - increased intracranial pressure - herniation - compromise of blood supply - hypoxia ischemia, infarction, irrecoverable brain damage and eventually death
Base of Skull Injury : Signs & Symptoms
Hemorrhage from the nose or ear (involvement of the middle ear of the frontal bone or paranasal sinuses
Blood may appear under the conjunctiva
Bruising may be seen in the mastoid area (Battle's sign)
CSF otorrhoea / rhinorrhoea
Halo sign - blood stain surrounded by a yellowish stain on the bed linen
Bloody CSF tap - suggests a brain laceration or contusion
Management of head injury
Assessment and Diagnostic findings
Evaluate neurologic status
X-ray skull AP and Lateral views
Take a CT scan
When needed MRI if the patient is stable enough
Nursing Management
Basal skull fractures are usually open and result in leak - the nasopharynx and the external ear kept clean - a sterile piece of cotton is placed in the ear or taped to the nose to absorb CSF
Coughing and sneezing avoided
Head elevated 30 degrees
Spontaneous closure of the leak is expected - if it is persistent surgery needed
Nursing Care Plan/Management of head injury with brain involvement
Assessment
Injury - When, How, Direction of force
H/O Loss of Consciousness - duration
Resposnse to verbal commands
Response to tactile stimuli
Pupils - size, equalness, speed of response
Glasgow Coma Scale
Corneal and gag reflexes
Motor and sensory functions
Assessment done periodically and compared
Nursing Diagnosis
Airway condition
Cerebral perfusion
Fluid and electrolyte status
Nutritional status
Seizures, disorientation, restlessness,
Temperature regulation impairment
Skin integrity
Hemiparesis, hemiplegia, immobility
Deficits in intellectual functions, communication, memory
Sleep pattern disturbances
Family support
Deficiency in knowledge
Intra cranial pressure
Collaborative Problems/Poteneial Complications
Decreased cerebral perfusion
Cerebral edema and herniation
Impaired oxygenation and ventilation
Impaired fluid and electrolyte balance
Deficits in nutrition
Seizures
Planning and Goals
Airway maintenance
Fluid and electrolyte balance
Adequate nutrition
Prevention of secondary injury
Maintenance of temperature
Maintaining skin integrity
Improving cognitive function
Proper sleep pattern
Coping by family
Teach rehabilitation
Teach about complications
Nursing Interventions
Maintain the airway - prevent falling back of tongue by insering an airway - clear secretions by suction - Before and after suctioning hyperoxygenate and hyperventilate to prevent hypoxia. put the patient in an appropriate position to prevent collection of secretions - prevent aspiration - maintain oral hygiene
Maintain breathing - if needed intubate/put on ventilator
Monitor neurologic functions - Level of consciousness - Glasgow coma scale - a score of 8 or less → severe head injury
Monitor vital signs
Look for increased Intra Cranial Pressure - bradycardia, increasing systolic blood pressure, widenint pulse pressure. Later respirations become rapid and BP may decrease
Monitor and maintain Temperature
Look for hidden bleeding elsewhere in the body
Motor functions assessed frequently e.g. strength of the limbs
Look for ability to move limbs and body
Differentiate from reflexive movements from voluntary motor response
Monitor Lab results
Maintain adequate nutrition
Prevent injury : restlessness may be due to hypoxia, fever, pain or a full bladder, catheter, iv lines. Provide padded side rails, if possible avoid restraints which may increase Intra cranial pressure
Avoid opioids
Safeguard from bed sores : appropriate bed, position changing, provide skin care, if possible sit the patient in a chair 3 times a day.
Minimize environmental stimuli : room quiet, limit visitors, provide adequate lighting to prevent visual hallucinations
Lubricate the skin to minimize irritation by bed sheets
Prefer intermittent catheterization of the bladder
Arrange consultation with neuropsychologist to improve cognitive, psychiatric and emotional problems
Enable the family to cope up with the situation
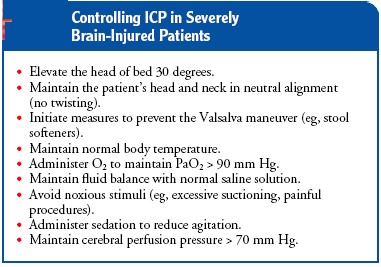
Monitoring and Managing Potential Complicatons
Maintain adequate CPP (Cerebral Perfusion Pressure) - Elevation of the head of the bed & increased IV fluids i.e. decreasing cerebral edema and increasing circulatory volume
Prvent Edema and Herniation
Control ICP by appropriate measures
Look for seceondary complications - diabetes insipidus which will need fluid and electrolyte replacement and vasopressin
Expected Patient Outcomes
Maintenance of patent airway
Attainment of optimal breathing pattern - normal ABG (arterial blood gas)
Optimal cerebral perfusion
Improvement of orientation, follow commands, answer correctly
Normal fluid and electrolyte balance
Absence of infections
Normal temperature
No complications - normal ICP, normal kidney function